
Ultrasound Guidance Importance: Lumbar Puncture
May 23, 2021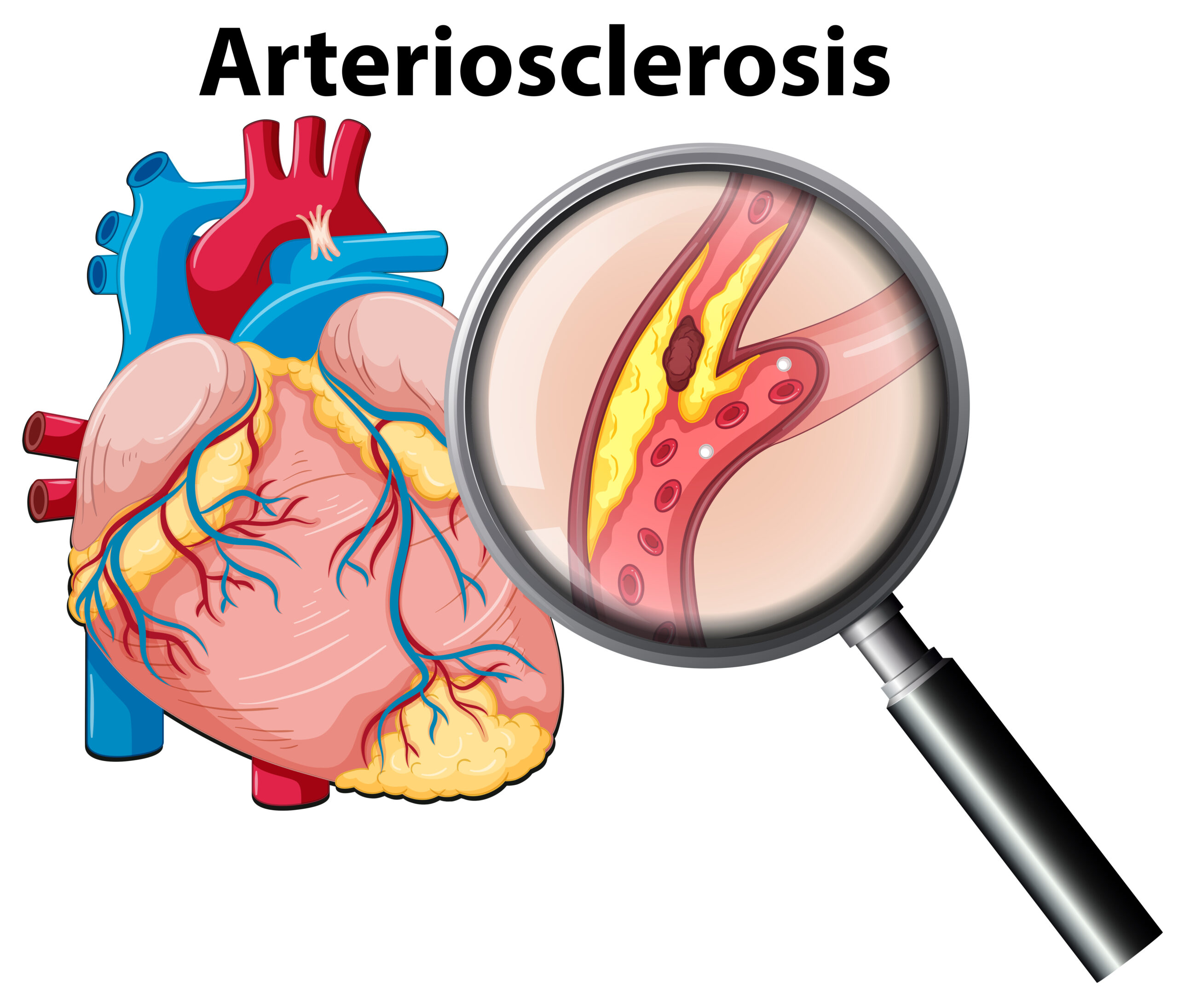
Arteriosclerosis
May 25, 2021
Hypertrophic pyloric stenosis is blockage of the passage out of the stomach due to thickening (hypertrophy) of the muscle at the junction between the stomach and the intestines.
Ultrasound (US) is the preferred diagnostic modality as it is a non-invasive technique, allowing direct observation of the pyloric canal morphology and behavior. It is important to carry out a systematic and dynamic study and to be aware of the common technical difficulties and how to overcome them.
Which Ultrasound is best for Hypertrophic pyloric stenosis diagnosis?
Ultrasound examination allows the gastroenterologists or the radiologist to perform a brief clinical history, which can reveal essential clues to the diagnosis. Yet, a high-frequency transducer Color Linear Ultrasound Scanner L7CD adjusted to the size of the patient, and the depth of the pylorus should be used. The 5 to 10 MHz linear probe will provide the depth required to visualize the pylorus.
In HPS the thickened muscle and elongated pylorus are fixed over time, which helps the operator to identify this condition. The appearance of the hypertrophied pylorus has been described as the cervix sign, as it resembles the appearance of the uterine cervix.
The Ultrasound allows a dynamic study with direct observation of the pyloric canal morphology and behavior. Most importantly, it should be performed by an experienced specialist. Having a systematic approach will improve the sensitivity of the technique.
A further US examination may be requested if vomiting persists following surgery. However, the radiologist and the surgeon should be aware that the pyloric muscle may remain thickened after successful surgery and can take up to 5 months to return to normal thickness.
Pyloric US examination is a dynamic investigation, which should be performed in a systematic way. The practitioner should be aware of the pitfalls of the examination and how to overcome them. It is important to be familiar with the normal and hypertrophied pyloric appearances, as this will provide greater diagnostic confidence, assisting in early diagnosis and improving the management of infants with HPS.
References: Hypertrophic pyloric stenosis, Pyloric Stenosis,

Disclaimer: Although the information we provide is used by different doctors and medical staff to perform their procedures and clinical applications, the information contained in this article is for consideration only. SONOSIF is not responsible neither for the misuse of the device nor for the wrong or random generalizability of the device in all clinical applications or procedures mentioned in our articles. Users must have the proper training and skills to perform the procedure with each ultrasound scanner device.
The products mentioned in this article are only for sale to medical staff (doctors, nurses, certified practitioners, etc.) or to private users assisted by or under the supervision of a medical professional.



{kind=link}
{kind=link}
{kind=link}